Clinical Summary
A 35-year-old asymptomatic woman presents to her gynecologist for a routine pelvic exam. The gynecologist notes fullness within the pelvis and orders a magnetic resonance imaging (MRI) of the abdomen and pelvis. On T2-weighted images, a large mass with a hyperintense signal is present in the deep soft tissue of the pelvis. It measures 10 cm in greatest dimension and encircles the rectum and bladder without obvious invasion. There is abutment of the pelvic sidewall but no apparent infiltration into the adjacent soft tissue.
Following surgical resection, gross examination demonstrates a tan-pink, poorly circumscribed, unencapsulated and multilobulated mass. Cut sections reveal a soft and gelatinous neoplasm with multifocal areas of hemorrhage. Small fragments of skeletal muscle and adipose tissue are identified at the periphery.
Master List of Diagnoses
- Aggressive angiomyxoma
- Angiomyofibroblastoma
- Cellular angiofibroma
- Myxofibrosarcoma
- Myxoid liposarcoma
- Superficial angiomyxoma
Archive Case and Diagnosis
This case first appeared as Performance Improvement Program in Surgical Pathology (PIP) 2018, Case 15, and is aggressive angiomyxoma of the deep soft tissue of pelvis.
Criteria for Diagnosis and Comments
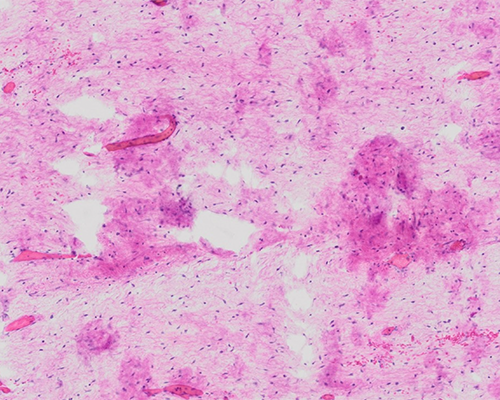
Histologic sections of the neoplasm reveal a hypocellular lesion with abundant myxoedematous stroma. Embedded within the myxoid stroma are numerous monomorphic spindled and stellate cells. The cells have small, bland nuclei and inconspicuous nucleoli. Mitotic figures are not identified. Also noted are numerous well-formed blood vessels of varying caliber, some of which are thickened and distinctly hyalinized. There is subtle infiltration of the neoplasm into the surrounding soft tissues, with entrapment of muscle, nerves, and fat.
Immunohistochemistry is performed, and the tumor cells express desmin, smooth muscle actin, vimentin, and CD34, but are negative for pan-cytokeratin and S100 protein. In addition, staining for estrogen and progesterone receptors (ER/PR) shows strong, diffuse positivity for both markers throughout the neoplasm. These findings are morphologically and immunohistochemically consistent with a diagnosis of aggressive angiomyxoma (AA).
AA is a relatively rare mesenchymal tumor that occurs most frequently in adult women of childbearing age, although a small subset of cases occurs in older women. This lesion shows a strong predilection for females over males, with a ratio of 6 females to 1 male. It is a site-restricted neoplasm that tends to arise in the deep soft tissues of the pelvic or perineal regions, often presenting as an asymptomatic mass discovered incidentally on physical exam or imaging. Occasionally AA can also produce clinical complaints of a perineal, vulvar, or scrotal mass, the extent of which is not fully appreciated until imaging reveals deep tissue or retroperitoneal extension.
On MRI, AA is classically a well-defined mass which displaces, rather than infiltrates, adjacent organs. It demonstrates hyperintense signaling on T2-weighted imaging due to the high water content and loose myxoid stroma. There is a characteristic pattern following intravenous contrast administration that is described as a heterogeneous layering or swirling, which is attributed to the internal vascularity of the neoplasm.
A recurrent translocation involving the high mobility group A (HMGA2) gene locus on chromosome 12 has been identified in up to 90% of AAs. HMGA2 overexpression can, therefore, be a useful discriminatory marker, as most neoplasms which closely mimic AA do not harbor this translocation. However, caution should be exercised as a few other vulvovaginal mesenchymal lesions, especially, but not exclusively, leiomyomas can be HMGA2-positive. The translocation can be detected either by fluorescent in situ hybridization (FISH) or via immunohistochemical staining of the encoded protein, which acts as a surrogate marker.
Because of its infiltrative pattern of spread, AA is often difficult to resect with clear margins. Radical resection can lead to significant morbidity, including infertility and bowel and bladder dysfunction. As most patients are younger women who often desire to retain their fertility, incomplete resection is often the procedure of choice. There have been limited reports of AA responding to hormonal therapy, either as neoadjuvant or postoperative treatment. Chemotherapy and radiation are of little utility due to the low mitotic activity of the neoplastic cells. As a benign tumor, recurrence and progression of AA are relatively indolent and often difficult to detect. According to the literature, up to 47% to 72% recur locally, often just a few years after excision.
The differential diagnosis of AA includes a number of morphologically similar mesenchymal neoplasms with a myxoid appearance including angiomyofibroblastoma (AMF), cellular angiofibroma, myxoid liposarcoma (MLS), myxofibrosarcoma (MFS), and superficial angiomyxoma. Many of these are composed of bland spindle cells which are immunoreactive for ER/PR, making the distinction between them quite challenging for surgical pathologists. The rarity of these lesions, coupled with the considerable morphologic and immunophenotypic overlap, result in great diagnostic difficulty. Despite this, histologic examination remains the mainstay in diagnosis, as immunohistochemistry is of extremely limited value. It is essential to establish a correct diagnosis, as the behavior and management of these lesions may differ markedly.
AMF occurs predominantly in women, same as AA, but has a later peak incidence than AA (4th and 5th decades). Both tumors are characterized by vasculature interspersed throughout loose stroma; however, AMF demonstrates more circumscribed borders, higher cellularity, and increased density of blood vessels. AMF may demonstrate significant stromal edema, causing it to appear very myxoid. The vessels of AMF may have perivascular sclerosis, although they lack the prominent hyalinization and/or hypertrophy of the walls, which characterize AA. The vascular component of AMF is always prominent, and is often intimately associated with the stromal cells, which tend to be plump, whereas those in AA are more spindled/stellate shaped with thin, delicate cytoplasmic processes. AMF is usually smaller (less than 5.0 cm) and more superficial in the vulvar region, in contrast to AA which is usually greater than 10 cm and arise in the deep paravaginal/pararectal soft tissues. AMF is not known to have HMGA2 overexpression, which can also be useful in the discrimination. AMF usually demonstrates positive immunohistochemical staining for ER and PR. Distinguishing between these two entities is vital, as treatment and prognosis for each is very different. For AMF, excision is curative, and it rarely recurs.
MLS comprises 5% to 10% of all adult soft tissue sarcomas and has a predilection for young adults, similar to AA. However, MLS occurs most commonly in the deep soft tissues of the extremities and is rarely seen in other sites such as the retroperitoneum. Histologically, MLS is characterized by an abundance of extracellular matrix material, and overall cellularity can be sparse (often resembling a “pulmonary edema” type of pattern) to moderately cellular. The defining features of MLS include the presence of lipoblasts, which often assume a “signet-ring” appearance, and the presence of a plexiform or arborizing type of capillary vasculature. The latter is in stark contrast to the disorganized larger and thick-walled vessels of AA. In limited studies, MLS has been distinguished from AA by immunohistochemical staining; AA is negative for S100 protein whereas MLS will show diffuse positivity. If present, cytogenetic abnormalities may also have utility in the distinction. Although MLS can have overexpression of HMGA2, it is also known to have t(12;16)(q13;p11), a fusion of DDIT3 gene locus (CHOP) to FUS or EWSR1, which has not been found in AA.
MFS is one of the more common soft tissue neoplasms of adults, rarely occurring in those less than 20 years of age. This lesion was formerly classified as a myxoid malignant fibrous histiocytoma but is now recognized as a distinct entity. Unlike AA, MFS is most common in the soft tissue of the extremities, with the lower extremities affected more often than upper. Histologically, MFS is classified as a low-, intermediate-, or high-grade. A low-grade lesion is the type most likely to be confused with an AA, as it tends to be lobulated, hypocellular with abundant extracellular matrix, and has scattered curvilinear vessels. Higher grade lesions should be recognized as such due to their frequent mitoses, necrosis, and pseudolipoblasts. These lesions are often desmin negative, unlike AA. MFS lesions are difficult to resect and often metastasize.
Cellular angiofibroma (CA) and AA have a slightly dissimilar demographic distribution, in that CA occurs equally in males and females, and often develops later in life. CA tends to originate in the superficial pelvic, perineal, and genital regions. CAs are well-circumscribed tumors and, in contrast to AA, rarely recur. CA may also be distinguished from AA by its higher cellularity, more fibrous (wiry collagen) stroma, and high density of hyalinized vessels. The vessels within the lesion often have intraluminal thrombi, which can lead to degenerative edematous changes, resembling a myxoid appearance. The presence of stromal mast cells or a mixed inflammatory response is more suggestive of CA than AA. In addition to the morphologic distinction, immunohistochemistry may be useful as CA is typically negative for smooth muscle markers and shows no HMGA2 overexpression. CA is also usually strongly positive for ER and PR.
Superficial angiomyxoma (SA) can involve the vulvovaginal region, but most often arises in the dermis and subcutaneous tissue of extragenital sites, especially the head and neck. SA is typically of smaller size than AA, lacks larger caliber vessels, and is characterized by a multinodular “pushing” growth pattern, rather than an invasive one. Additionally, stromal neutrophils are often identified in SA, but are not a finding associated with AA. SA typically stains negatively for ER, PR, and desmin, all of which are expected to be strongly positive in an AA.
Supplementary Questions
- Which of the following clinical scenarios best describes a classic presentation of an aggressive angiomyxoma?
- An 8-year-old boy with a superficial, subcutaneous vascular lesion in the lateral neck.
- A 17-year-old boy with a rapidly growing mass in the retroperitoneum and lung nodules.
- A 20-year-old woman with an invasive pelvic mass and enlarged regional lymph nodes.
- A 37-year-old woman with a slow-growing, painless perineal mass.
- A 63-year-old man with a deep, painful soft tissue mass in the proximal thigh.
- Which of the following proteins is overexpressed in greater than 90% of aggressive angiomyxomas?
- FGFR2
- HER2
- HMGA2
- MDM2
- WT1
- Which of the following histologic features are most consistent with an aggressive angiomyxoma?
- Hypercellularity, edematous stroma, plump stromal cells, prominent vessels with perivascular sclerosis.
- Hypercellularity, fibrous stroma with wiry collagen, high density of hyalinized vessels with intraluminal thrombi, mixed inflammatory response.
- Hypocellularity, myxoedematous stroma, monomorphic spindled cells, well-formed and hyalinized blood vessels of varying caliber.
- Hypocellularity, myxoid stroma, high grade spindled cells, frequent mitoses, areas of necrosis.
- Sparse to moderate cellularity, “pulmonary edema” pattern, lipoblasts, plexiform/arborizing capillary vasculature.
References
- Calonje E, Guerin D, McCormick D, Fletcher CD. Superficial angiomyxoma: clinicopathologic analysis of a series of distinctive but poorly recognized cutaneous tumors with tendency for recurrence. Am J Surg Pathol. 1999;23(8):910-917.
- Chan YM, Hon E, Ngai SW, Ng TY, Wong LC. Aggressive angiomyxoma in females: is radical resection the only option? Acta Obstet Gynecol Scand. 2000;79:216-220.
- Dreux N, Marty M, Chibon F, et al. Value and limitation of immunohistochemical expression of HMGA2 in mesenchymal tumors: about a series of 1052 cases. Mod Pathol. 2010;23(12):1657-1666.
- Fetsch JF, Laskin WB, Tavassoli FA. Superficial angiomyxoma (cutaneous myxoma): a clinicopathologic study of 17 cases arising in the genital region.
Int J Gynecol Pathol. 1997;16(4):325-334.
- Fletcher CD, Tsang WY, Fisher C, Lee KC, Chan JK. Angiomyofibroblastoma of the vulva. A benign neoplasm distinct from aggressive angiomyxoma. Am J Surg Pathol. 1992;16(4):373-382.
- Iwasa Y, Fletcher CD. Cellular angiofibroma: clinicopathologic and immunohistochemical analysis of 51 cases. Am J Surg Pathol. 2004;28(11):1426-1435.
- Kairi-Vassilatou E, Dastamani C, Vouza E, Mavrigiannaki P, Hasiakos D, Kondi-Pafiti A. Angiomyofibroblastoma of the vulva: a clinicopathological and immunohistochemical analysis of a rare benign mesenchymal tumor. Eur J Gynaecol Oncol. 2011;32(3):353-355.
- Kazmierczak B, Wanschura S, Meyer-Bolte K, et al. Cytogenic and molecular analysis of an aggressive angiomyxoma. Am J Pathol. 1995;147(3):580-585.
- Lee CH, Ali R, Gilks CB. Molecular genetics of mesenchymal tumors of the female genital tract. Surg Pathol Clin. 2009;2(4):823-834.
- McCluggage WG. A review and update of morphologically bland vulvovaginal mesenchymal lesions. Int J Gynecol Pathol. 2005;24(1):26-38.
- Nucci MR, Granter SR, Fletcher CD. Cellular angiofibroma: a benign neoplasm distinct from angiomyofibroblastoma and spindle cell lipoma. Am J Surg Pathol.1997;21(6):636-644.
- Rabban JT, Dal Cin P, Oliva E. HMGA2 rearrangement in a case of vulvar aggressive angiomyxoma. Int J Gynecol Pathol.
2006;25(4):403-407.
Authors
Renée L Betancourt, MD
Pathology Resident
University of North Carolina
Chapel Hill, NC
Leslie G Dodd, MD
Surgical Pathology Committee
University of North Carolina
Chapel Hill, NC
Answer Key
- A 37-year-old woman with a slow-growing, painless perineal mass. (d)
- HMGA2 (c)
- Hypocellularity, myxoedematous stroma, monomorphic spindled cells, well-formed and hyalinized blood vessels of varying caliber. (c)