Clinical Summary
A 70-year-old woman with a long history of smoking presents with weight loss, cough, and shortness of breath of several months’ duration. A chest radiograph shows a large dense opacity in the right upper lobe with traction of the minor fissure and hilar adenopathy. Computed tomography scan reveals a 12 cm mass with enlarged hilar lymph nodes. Mediastinoscopy is negative. Right upper lobectomy along with mediastinal lymph node dissection is performed. Gross examination reveals a 12.5 cm yellow-white mass with central cavitation that seems to be invading into the visceral pleura, causing retraction. The tumor is positive for cytokeratin 5/6 and p63 and negative for TTF-1, Napsin A, HMB-45, SOX-10, cytokeratin 7, and cytokeratin 20.
Master List of Diagnoses
- Large cell carcinoma
- Melanoma
- Pleomorphic carcinoma
- Poorly differentiated adenocarcinoma
- Poorly differentiated squamous cell carcinoma
Archive Case and Diagnosis
This case first appeared as Performance Improvement Program in Surgical Pathology (PIP) 2019, Case 06, and is poorly differentiated squamous cell carcinoma of the lung.
Criteria for Diagnosis and Comments
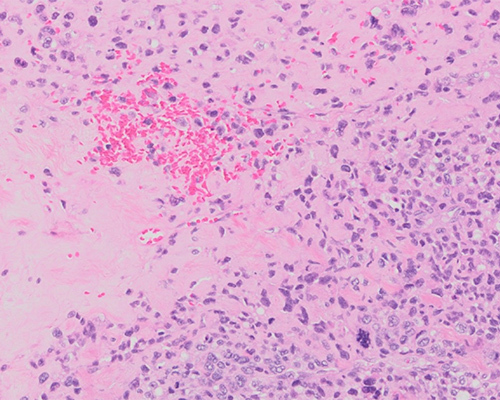
Histologic sections show sheets or nests of large polygonal cells with vesicular nuclei, prominent nucleoli, and a moderate amount of cytoplasm. On most slides, the tumor shows characteristics of a non-small cell lung carcinoma (NSCLC); however, some slides show focal squamous differentiation. In these cases, it is important to perform immunostains to confirm squamous differentiation and exclude adenocarcinoma or adenosquamous carcinoma, as those diagnoses would warrant further molecular testing. The tumor cells express p40, CK5/6 and p63 (markers for squamous cell carcinoma) and negative for TTF-1 and Napsin A (markers for lung adenocarcinoma), confirming the diagnosis of poorly differentiated squamous cell carcinoma.
Squamous cell carcinoma (SCC) is a malignant epithelial tumor showing keratinization and/or intercellular bridges that arises from bronchial epithelium. More than 90% of squamous cell lung carcinomas occur in cigarette smokers. The majority of squamous cell lung carcinomas arise centrally in the mainstem, lobar, or segmental bronchi. The primary tumor and its central extent of disease is usually best demonstrated by CT scan. The cytology of tumor cells depends on the histologic differentiation and type of sampling. On cytologic smears, the tumor cells may occur singly or in clusters and may show bizarre shapes such as spindle-shaped and tadpole-shaped cells. Cohesive aggregates may occur in flat sheets with elongated or spindled cells. On histologic examination, squamous cell carcinoma shows keratinization, pearl formation, and/or intercellular bridges. These features vary with degree of differentiation, being prominent in well-differentiated tumors and focal in poorly differentiated tumors.
On gross examination, SCC are usually white or grey and, depending on the severity of fibrosis, firm with focal carbon pigment deposits in the center and retractions at the periphery. The tumor may grow to a large size and may cavitate. Central tumors form intraluminal polypoid masses and/or infiltrate through the bronchial wall into the surrounding lung parenchyma, occluding the bronchial lumen and resulting in stasis of bronchial secretions, atelectasis, bronchial dilatation, obstructive lipoid pneumonia, and bronchopneumonia. A minority of cases may arise in small peripheral airways.
Detection of aneuploidy by DNA measurement has been shown to be a poor prognostic factor for SCC of the lung. ErbB (EGFR, HER2, KRAS) pathway abnormalities are common in non-small cell carcinoma but absent in SCC. Stage for stage, the survival rate for SCC is significantly better than for adenocarcinoma. Approximately 80% of patients with resected stage 1 (T1 N0 M0) SCC are alive at 5 years after diagnosis compared to approximately 70% of similarly staged adenocarcinomas.
Large cell carcinoma (not to be confused with large cell neuroendocrine carcinoma) is an undifferentiated non-small cell carcinoma that lacks the cytologic and architectural features of small cell carcinoma and glandular or squamous differentiation. Large cell carcinoma accounts for approximately 9% of all lung cancers. It is a diagnosis of exclusion made after ruling out the presence of a component of SCC, adenocarcinoma, or small cell carcinoma. Large cell carcinomas share the molecular and genetic alterations commonly seen in NSCLC, since it is a poorly differentiated tumor arising from the same stem cells, exposed to the same carcinogens. KRAS mutations, TP53 mutations and Rb pathway alteration (loss of p16INK4, hyperexpression of cyclin D1 or cyclin E) occurs with the same frequency as in other NSCLC.
Melanoma metastasizing to the lung is in the differential diagnosis of these tumors, especially when cytokeratin immunostaining is negative. In these situations, performing HMB-45, SOX-10, and Melan-A is helpful for diagnosis.
Pleomorphic carcinoma is a rare, poorly differentiated subtype of lung carcinoma defined by the 2021 World Health Organization Classification as a squamous cell carcinoma, adenocarcinoma, and/or large cell carcinoma that contains at least 10% spindle and/or giant cells, or a carcinoma consisting only of spindle and/or giant cells. While the presented case is poorly differentiated, no significant spindle or giant cell component is noted; therefore, it does not meet criteria for diagnosis of pleomorphic carcinoma.
Poorly differentiated adenocarcinoma or the solid variant of lung adenocarcinoma is composed of sheets of polygonal cells lacking acini, tubules, and papillae, but with mucin present in at least 5 tumor cells in each of 2 high-power fields, confirmed with histochemical stains for mucin. Squamous carcinomas and large cell carcinomas of the lung may show rare cells with intracellular mucin, but this does not indicate classification as adenocarcinoma. These tumors express cytokeratin 7, TTF-1 and Napsin A. TTF-1 is especially positive in the better differentiated tumors. Common genetic alterations include EGFR, KRAS and BRAF mutations; translocation of ALK, ROS1, and RET; and amplification of MET and FGFR1.
Supplementary Questions
- Which of the following is most distinctive of poorly differentiated squamous cell carcinoma (SCC)?
- Immunoreactivity for p63 and p40
- Immunoreactivity for HMB-45
- Presence of necrosis
- Translocations involving chromosome 12
- Tumor cells forming glands
- Which of the following is true of poorly differentiated lung SCC?
- Distant metastases are not seen.
- Prognosis is independent of stage.
- Stage for stage, survival rate is significantly better than for adenocarcinoma.
- These tumors show large areas of keratinization.
- Tumor cells express TTF-1.
- Which of the following is most typical of lung adenocarcinoma?
- Common alterations include EGFR, KRAS, and BRAF
- Express p63 and p40
- Grossly well-circumscribed
- Least commonly seen in the periphery of the lung
- Most are central tumors
References
- Lindeman NI, Cagle PT, Beasley MB, et al. Molecular testing guideline for selection of lung cancer patients for EGFR and ALK tyrosine kinase inhibitors: guideline from the College of American Pathologists, International Association for the Study of Lung Cancer, and Association for Molecular Pathology. J Thorac Oncol. 2013;8(7):823–859.
- Rekhtman N, Paik PK, Arcila ME, et al. Clarifying the spectrum of driver oncogene mutations in biomarker-verified squamous carcinoma of lung: lack of EGFR/KRAS and presence of PIK3CA/AKT1 mutations. Clin Cancer Res. 2012;18:1167–1176.
- Tsao MS, Znaor A, Travis WD, et al., editors. Tumours of the Lung. In: WHO Classification of Tumors Editorial Board. Thoracic Tumours. 5th ed. International Agency for Research on Cancer, Lyon, FR: International Agency for Research on Cancer; 2021.
Author
Kirtee Raparia, MD
Surgical Pathology Committee
Kaiser Permanente Medical Center
Santa Clara, CA
Answer Key
- Immunoreactivity for p63 and p40 (a)
- Stage for stage, survival rate is significantly better than for adenocarcinoma. (c)
- Common alterations include EGFR, KRAS, and BRAF (a)